The Hard 30%: From Signals to Decisions
Building high-integrity decision support in care-critical, regulated environments
Outcome focus: trustworthy decisions, reduced cognitive load, compliance by design
This is about the hard 30% of product delivery. Care-critical systems demand trust, not dashboards. Regulation, human judgement, and delivery discipline intersect here.
Most product work lives in the comfortable 70%—features, flows, nice-to-haves. The hard 30% is where lives and livelihoods depend on decisions made with your product. Where compliance isn't a checkbox but a precondition. Where the goal isn't more data but confident action.
This case is anonymised and imaginary, inspired by real challenges in care-critical, regulated product environments. The patterns are real. The specifics are composite.
Start with the Outcome, Not the Output
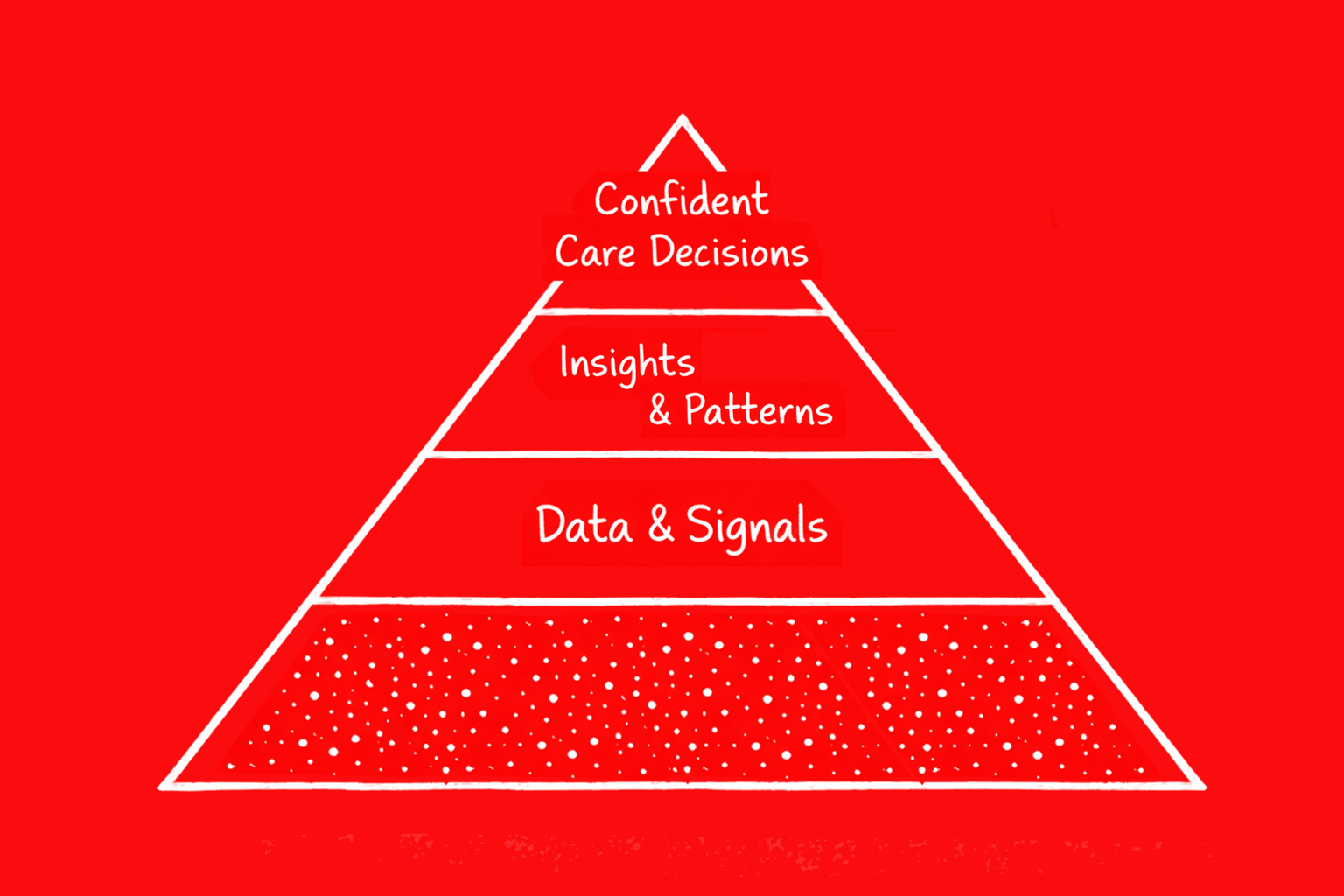
Outcomes over features. Decision confidence over data volume. Usage metrics are insufficient in care-critical systems—a clinician who logs in daily but hesitates to act on a recommendation hasn't been served. The product failed even if the dashboard looked busy.
The North Star for this domain is not "daily active users" or "features adopted." It is:
Confident, timely care decisions that improve resident outcomes without increasing staff burden.
Everything else—dashboards, alerts, reports—ladders up to that. If it doesn't increase decision confidence or reduce burden, it's noise.
Mapping the Value Landscape
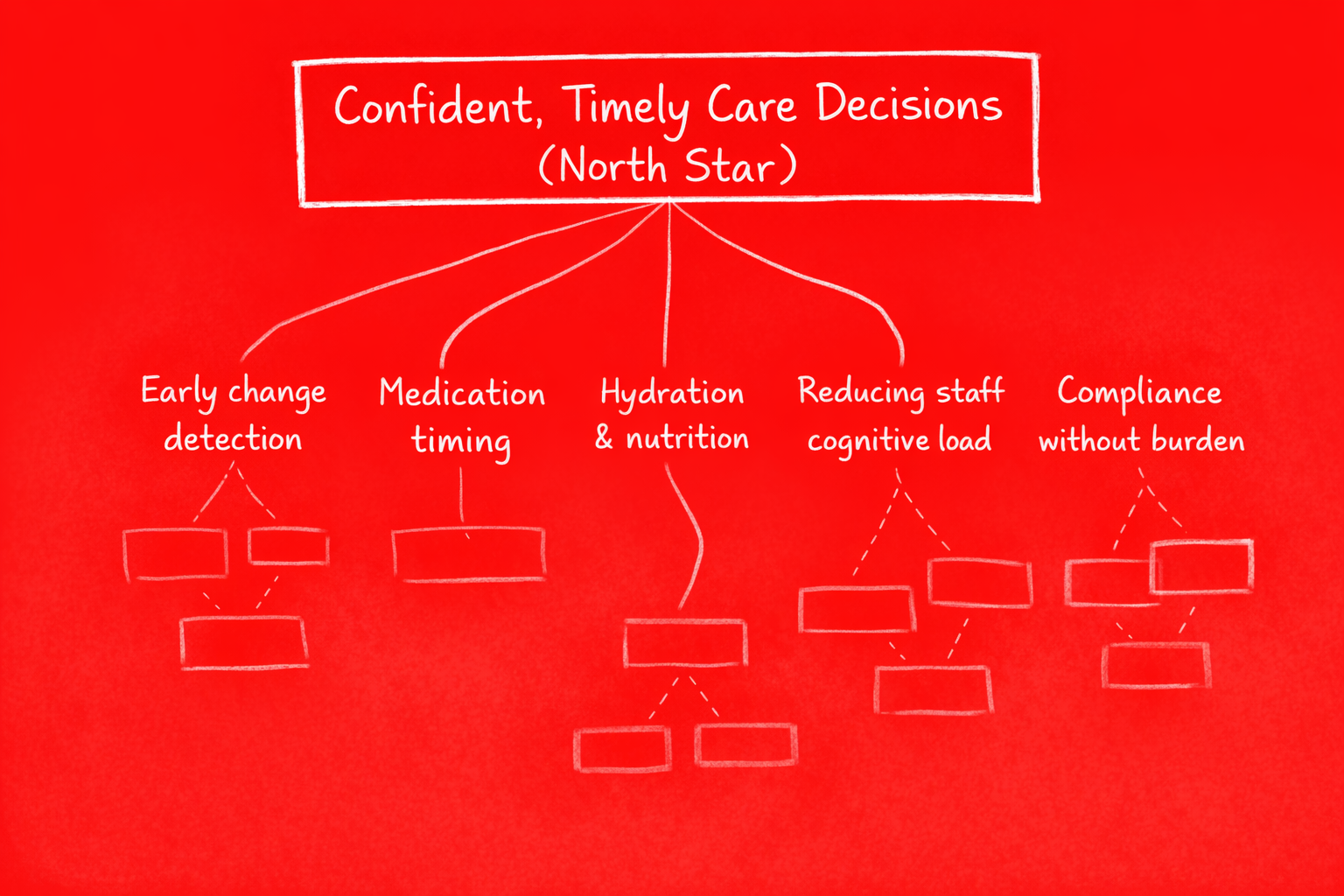
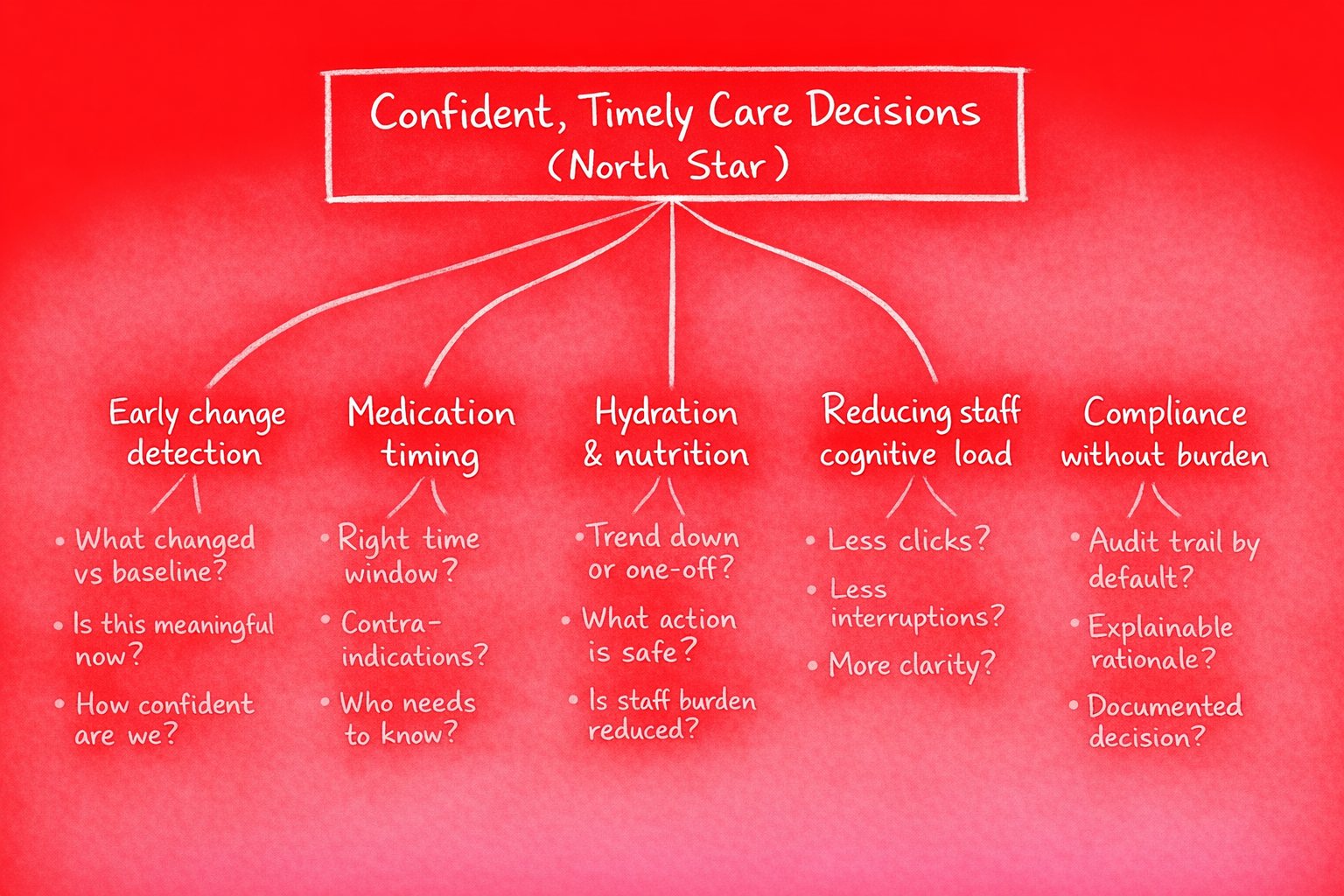
The Opportunity Solution Tree puts the North Star at the top. Beneath it sit opportunity areas: hydration, medication timing, early deterioration signals, cognitive load, compliance. Solutions are intentionally de-emphasised. The map is about where value lives, not what to build first.
In regulated environments, opportunity mapping matters more than solution ideation. You need to know which problems are worth solving before you commit to a solution that will require audits, validation, and human-in-the-loop design. Jump to solutions too early and you burn cycles on the wrong thing.
The Job to Be Done (JTBD)
Frame this as a socio-technical system, not a single "user." The primary job is: make care decisions that improve outcomes while staying within regulatory and workflow constraints.
- Primary job: Support confident, timely care decisions that improve resident outcomes
- Beneficiary: The resident receiving care
- Actor: Care staff and clinicians who notice, decide, and act
- Decision maker: Clinician or care lead who validates and owns the decision
- Accountable party: Provider organisation carrying regulatory and outcome responsibility

The product serves the actor and the decision maker. The beneficiary's outcome is the measure of success. The accountable party must trust that the system supports, not replaces, human judgement.
Breaking the Decision into Steps
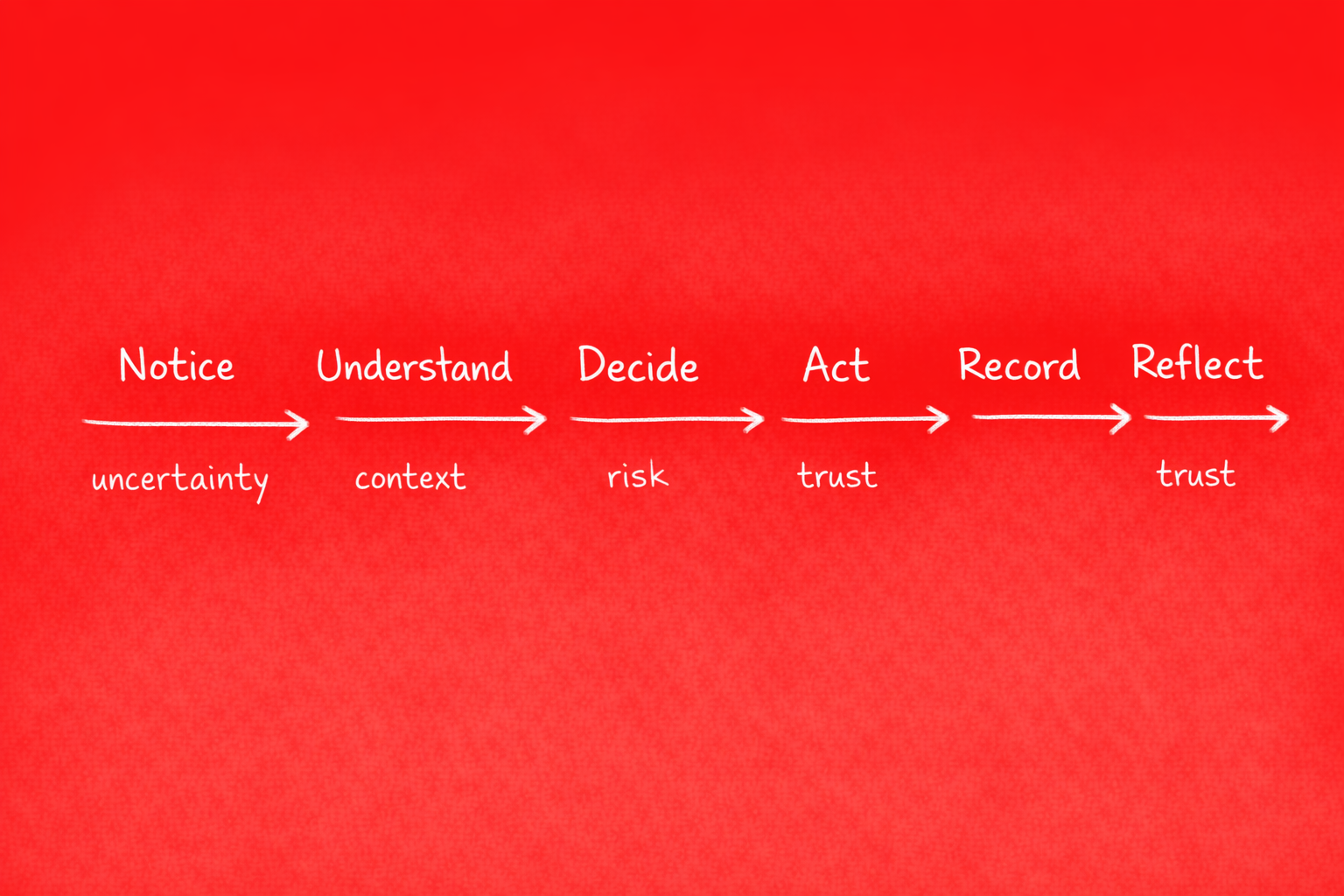
The care decision journey has six steps: Notice, Understand, Decide, Act, Record, Reflect. Most products overload steps 2 and 4—they dump data at Understand and push alerts at Decide. The result is cognitive overload and alert fatigue.
- Notice: Something signals attention—a trend, a threshold, a pattern
- Understand: Context and rationale, not raw data. What does this mean? Why does it matter?
- Decide: Clear options with trade-offs. Framed for action, not ambiguity
- Act: Execute the decision within workflow
- Record: Documentation for compliance and continuity
- Reflect: Learn from outcomes to improve future decisions
Products that win focus on reducing friction at Understand and Decide. They don't add more dashboards. They add clarity.
The Real Competition
The competition isn't other software. It's paper notes, intuition and experience, basic alerts, retrospective reports, and workarounds outside systems. Clinicians already have ways to make decisions. Your product must fit into that reality.
Trust and workflow fit beat sophistication. A simple, reliable prompt that fits the moment beats a complex dashboard that requires interpretation. The bar is high: you're asking people to change behaviour in high-stakes environments. They will only do that if the product earns trust incrementally.
Doing It Better (Not Louder)
Win with decision framing over alerts. Context and rationale over prediction. Human-in-the-loop by design. Compliance as an input, not a gate.
- Decision framing: Present options with trade-offs, not just "something changed"
- Context and rationale: Explain why a recommendation matters, not just what it is
- Human-in-the-loop: Every decision is validated by a human. The system supports; it doesn't replace
- Compliance as input: Build audit trails and documentation into the flow, not as an afterthought
Pragmatic and grounded. No AI hype. No "disruption." Just better decisions, made with confidence.
The First Product Increment
Start deliberately narrow. One decision. One workflow. One role. One outcome.
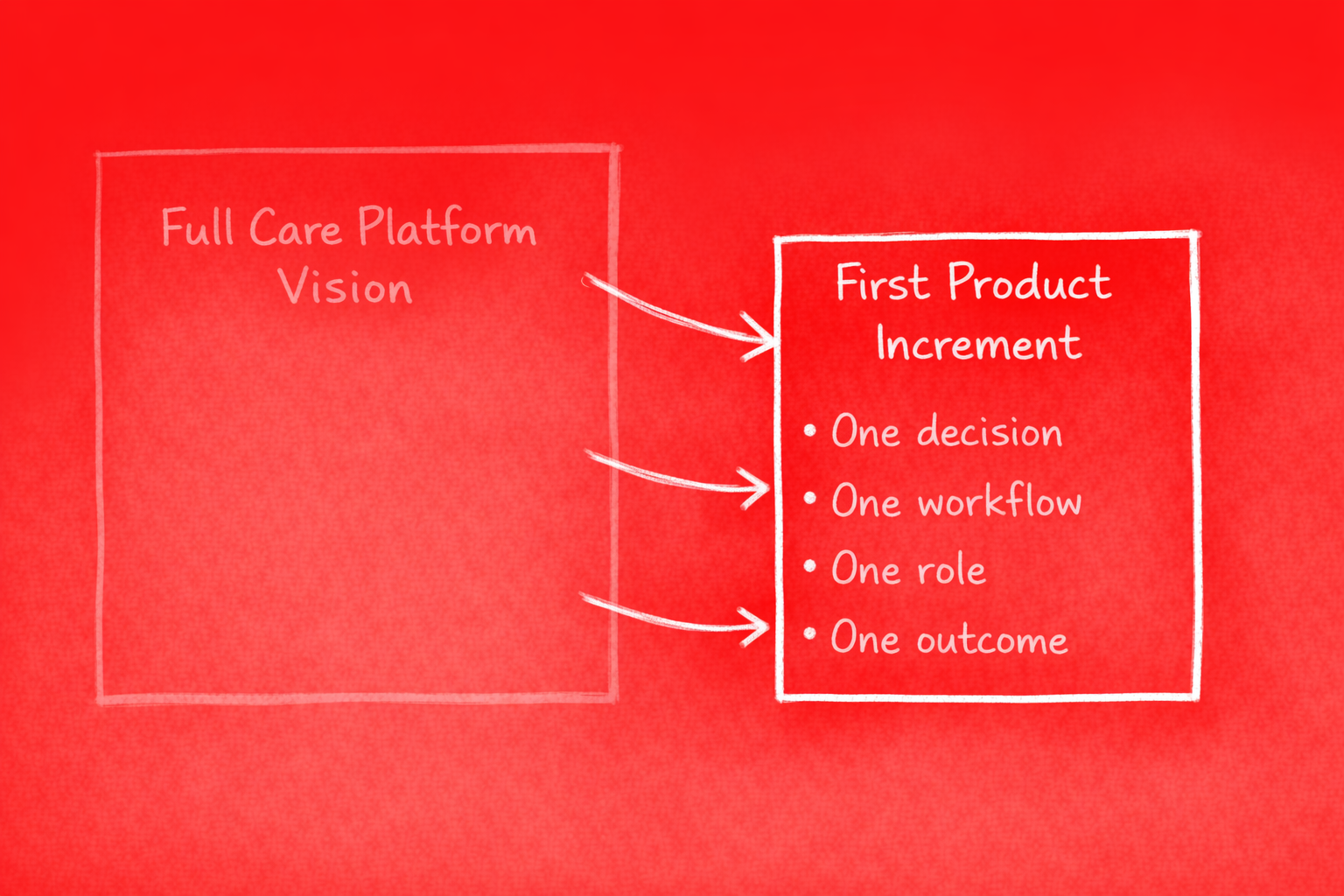
Example: hydration-related care decisions. A single class of decisions with clear inputs (intake, output, trends), a defined actor (care staff), a clear decision point (when to escalate, when to adjust), and a measurable outcome (resident hydration status, incident reduction).
Prove the pattern works. Then extend. Scaling from one decision to a platform is a feature of disciplined sequencing, not big-bang delivery.
Build – Measure – Learn (in a Regulated Reality)
Experimentation works, but it has to be safe. Build: auditable, co-designed, compliant. Measure: decision acted on, trust signals—not vanity metrics. Learn: where confidence breaks down and why.
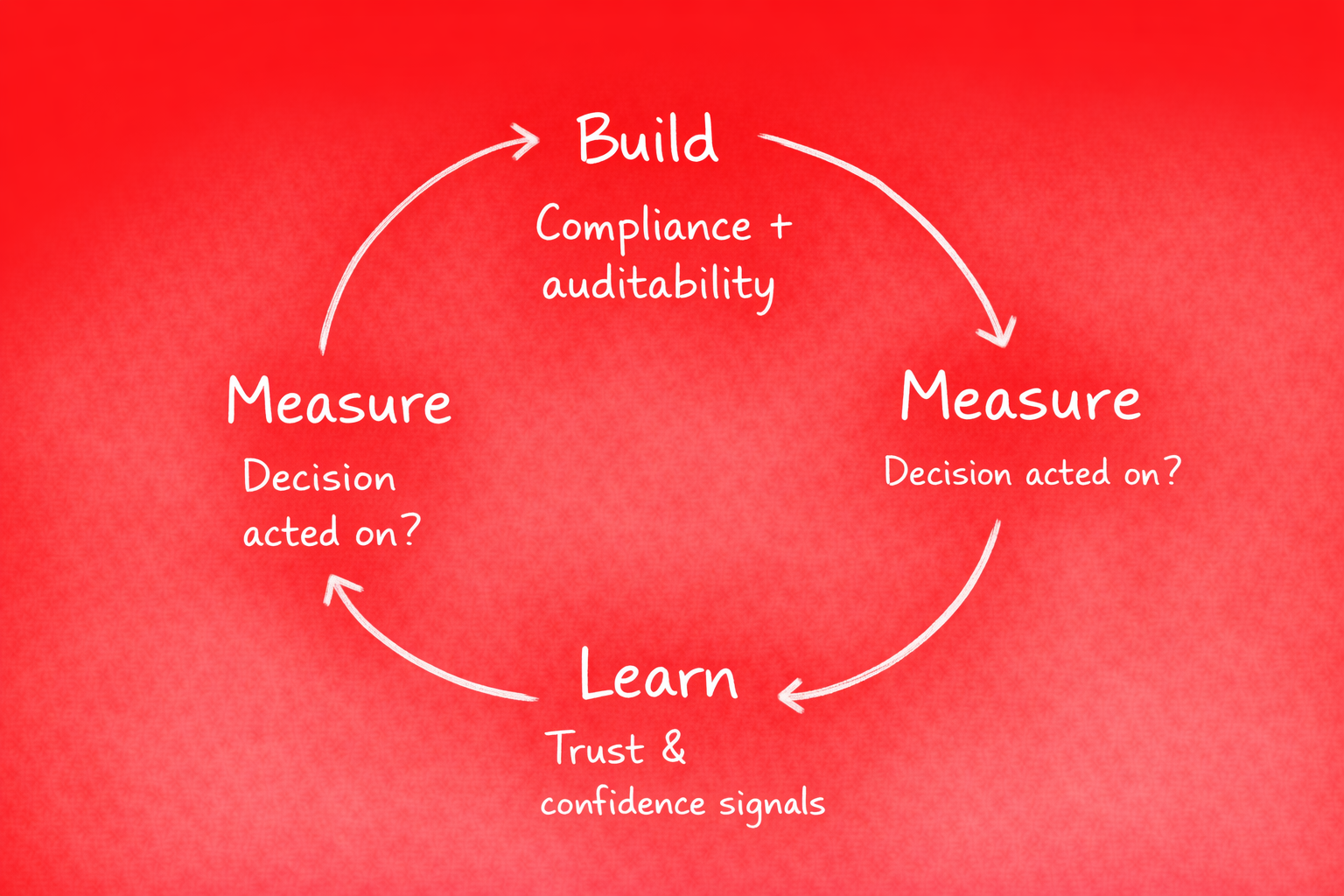
This is about learning speed without sacrificing safety. Hypothesis-driven iteration within guardrails. You're not A/B-testing clinical outcomes; you're testing whether the decision support lands. Whether clinicians trust it. Whether it fits the workflow.
Why This Works
This approach respects human judgement. It reduces cognitive load by framing decisions, not dumping data. It builds trust incrementally, one decision at a time. It scales from one decision to a platform because the pattern is repeatable.
Care-critical products don't win on features. They win on being quietly reliable. On fitting. On earning trust through consistent behaviour.
Closing
Care-critical products win by being quietly reliable. The hardest work isn't flashy. There are no viral moments, no growth hacks. This is where meaningful impact is created—in the decisions that get made, the outcomes that improve, and the trust that gets earned.
This case is anonymised and imaginary, inspired by real care-critical, regulated product challenges. Details have been adapted for publication.